What is acute myeloid leukemia (AML)?


Acute myeloid leukemia, also known as acute myeloblastic leukemia, acute myelogenous leukemia, acute granulocytic leukemia, but more commonly as AML, is the most common type of acute leukemia in adults.
Under normal conditions, a person’s bone marrow produces cells called myeloblasts that, after maturation, become granulocytes, which are the cells responsible for defending the body against infections. However, in patients with Acute myeloid leukemia, the myeloblasts proliferate abnormally, progressively invading the bone marrow and interfering with the normal production of blood cells.
Occasionally, acute myeloid leukemia is but the final stage of other diseases such as myelodysplastic syndromes or chronic myeloproliferative syndromes. The incidence of AML is very high among patients with certain chromosomal alterations such as Down syndrome or Fanconi Anemia.
AML may appear years after receiving chemotherapy or radiation therapy for the treatment of types of cancer. In these cases, the AML is considered secondary. It is an adult disease, although it can sometimes be observed in children.
How frequent is acute myeloid leukemia?


This type of leukemia accounts for 40% of all cases of leukemia in the western hemisphere. More than 20,000 new cases are diagnosed every year, resulting in more than 10,000 deaths.
Acute myeloid leukemia is a relatively rare disease compared to other types of cancer. However, according to most estimates, every year, between 3 to 4 new cases of acute myeloid leukemia are diagnosed per 100,000 inhabitants.
The median age for the diagnosis of acute myeloid leukemia is 65 years. It is very infrequent in patients below the age of 45, and as such, it is considered a type of cancer more typical of old age.
The probability of developing the disease increases with every passing decade. Therefore, the probability that a patient between 70 and 85 years of age develops AML is significantly higher than the probability of a patient who is between the ages of 50 to 70.
Another curious fact is that acute myeloid leukemia is somewhat more common in men than in women, with a ratio of 1.3 men diagnosed for each woman.
Pathophysiology of acute myeloid leukemia


AML is caused by malignant myeloblast formation. In the normal process of blood cell formation, the myeloblast is a young antecedent of the myeloid lineage of white blood cells. A normal myeloblast will eventually transform to become one of the many types of mature white blood cells. However, in cases of acute myeloid leukemia, the myeloblasts accumulate a series of mutations in their genomes that prevent them from continuing the normal process of cell differentiation. In other words, they become “frozen” in an immature state.
However, this condition is still not enough to produce leukemia. When other mutations of the genes that control cell proliferation are added to the absence of myeloblast differentiation, the result is an uncontrolled division of myeloblasts, which leads to the development of AML.
The symptoms of AML are caused by the uncontrolled proliferation of leukemic cells that displace healthy cells and disrupt the development of all other blood cell types that originate in the bone marrow. As the disease progresses, patients typically develop other disorders related to blood cell count, such as anemia, neutropenia, and thrombocytopenia.
Acute myeloid leukemia symptoms


Bone marrow failure and infiltration of internal organs with aberrant cells causes the majority of signs and symptoms in acute myeloid leukemia. Others result from complications derived upon the pathophysiology of the disease. Younger patients usually start displaying symptoms after a few days or after one or two weeks. Others may start with prodromal symptoms for weeks or months before acute and more severe symptoms start to appear.
In acute myeloid leukemia, we are expected to see the following signs and symptoms:
1) Fatigue

It is one of the most common and the majority of patients display fatigue for some time before the onset of more severe symptoms. There are many causes for this fatigue, including an increase in the metabolic rate and anemia (a reduction of red blood cells) that results from the disease.
2) Dyspnea and chest pain


Many patients describe a difficulty to take deep breaths and getting tired easily. In some cases, these symptoms are accompanied with dizziness, and patients with previous heart problems may have chest pain and may even have a heart attack as the first symptom of acute myeloid leukemia.
3) Fever

It is a key symptom to diagnose acute myeloid leukemia. Since fever usually points out to infection, patients run blood tests and see an increased total white blood cell count with a low neutrophil count. Still infection is hardly traced, and it is cataloged as fever of unknown origin.
4) Propensity to infections

The lower neutrophil count is, the higher propensity to infection patients will have. The most common infections are located in the upper respiratory tract, and sometimes in the urinary system.
5) Hemorrhagic manifestations


Patients with acute myeloid leukemia have several blood problems, and that includes impaired coagulation. They may report bleeding gums or hemorrhagic manifestations in the skin, such as red dots called petechiae, and larger areas of skin hemorrhage, called ecchymoses. Some of them may start bleeding in the gastrointestinal tract, and undergo life-threatening situations when bleeding occurs in the central nervous system or the lungs.
6) Enlargement of the spleen

The most common place of infiltration of leukemic cells is the spleen, and the organ becomes large and induces early satiety. This can be noted in the physical examination or diagnosed with an ultrasound. Other places of infiltration include the gums, causing gingivitis and gum bleeding, and the liver, causing hepatomegaly or enlargement of the liver.
7) Enlarged lymph nodes

Lymph nodes are an important part of the immune system, and they are directly affected by acute myeloid leukemia. However, enlarged lymph nodes are not required for diagnosis, and some patients may not display this symptom.
8) Altered mental status

In some cases, there are so many white blood cells populating the blood that it becomes thick and very dense. This is called leukostasis, and in these cases, the circulation in the smallest arteries of the brain becomes impaired. Thus, patients start displaying respiratory distress and changes in their mental status that include confusion, lethargy, and coma. This is one of the most life-threatening situations in acute myeloid leukemia, and these patients require emergency medical attention to improve their prognosis.
Causes of AML


The pathogenesis of AML is still unclear, but a double mechanism has been suggested as a probable cause for leukemogenesis. That means that AML could be the consequence of at least two different types of acquired genetic mutations. While the exact cause of acute myeloid leukemia is unknown, a number of associated risk factors have been identified:
The risk factors associated with acute myeloid leukemia are:
1) Exposure to chemical agents


Some studies have determined that exposure to high doses of benzene increases the risk of developing acute myeloid leukemia. Benzene is a chemical that was previously used in industries that manufactured plastics, resins, and other chemicals. Although its use is not as prevalent as before, it is still widely used to make adhesives, lubricants, dyes, detergents, and pesticides. Various studies have been carried out to try to establish a connection between exposure to these substances in the work environment and the development of AML. Still, no conclusive data has yet been obtained.
2) Previous treatment for cancer


The most common treatment for some types of cancer is chemotherapy. Some of the drugs that are used in chemotherapy have been linked in a number of studies with an increased risk of developing acute myeloid leukemia. These drugs include alkylating agents, anthracyclines, epipodophyllotoxins, purine analogs, and platinum derivatives. Therefore, reducing the dose or number of chemotherapy agents that are used to treat these types of cancer has been suggested as a way to reduce the risk of developing AML. It is important to note that the risk of developing AML as a result of chemotherapy is significantly lower than the expected benefit of receiving chemotherapy for the curative treatment of another type of cancer.
3) Radiation exposure


Exposure to very high doses of radiation increases the risk of developing acute myeloid leukemia. Therefore, the treatment of another type of cancer with radiotherapy has been linked with a higher risk of developing AML.
4) Hematological Disorders
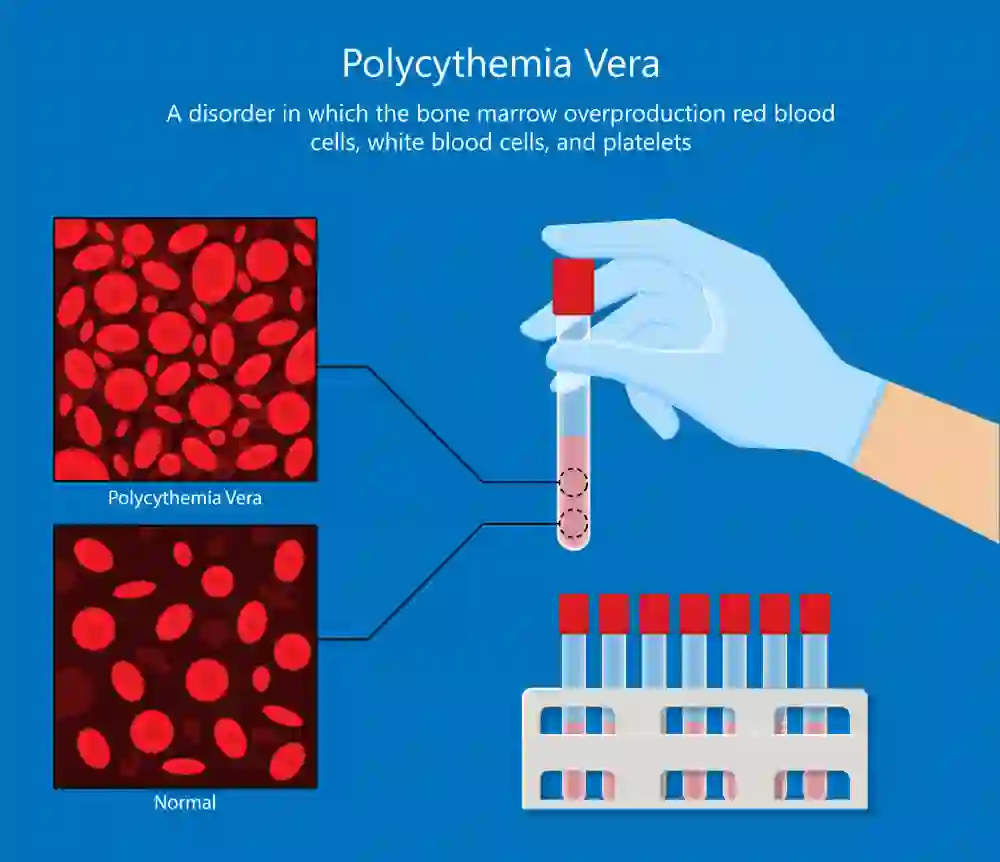

Patients with chronic myeloproliferative diseases such as polycythemia vera, essential thrombocythemia, or myelofibrosis are more likely to develop acute myeloid leukemia when compared to a healthy population, especially if chemotherapy or radiotherapy has been used as treatment. Having a myelodysplastic syndrome also increases the risk of developing acute myeloid leukemia.
5) Genetic syndromes


Some syndromes related to genetic or chromosomal mutations significantly increase the risk of developing acute myeloid leukemia. Among these disorders, we find down syndrome and other types of trisomy. Genetic diseases that cause defects in the repair of gene material such as Fanconi Anemia, Bloom syndrome, Louis–Bar syndrome, Blackfan-Diamond syndrome, Wiskot-Aldrich syndrome, Schwachman syndrome, Li-Fraumeni, neurofibromatosis, congenital neutropenia or Kostmann syndrome, also increase the risk of developing acute myeloid leukemia.
Prognosis of patients with AML

Acute myeloid leukemia is a curable disease. However, the prognosis of acute myeloid leukemia depends on a number of factors such as age, the general state of health, and the specific disease subtype. Depending on these factors, the probability of recovery of each patient changes.
To determine the prognosis of each patient, a number of prognostic factors are taken into account and evaluated against various treatment options.
Patient cytogenetics is one of the most important factors that are evaluated to obtain a reliable prognosis of the disease since there are certain chromosomal abnormalities closely related to specific subtypes of leukemia.
However, about half of patients with acute myeloid leukemia have normal cytogenetic profiles. These patients are considered to be in the intermediate-risk group. On the other hand, there are very specific cytogenetic abnormalities that are associated with an adverse prognosis, since they present the highest risk of relapse after treatment.
Cases of AML that have arisen from a preexisting myelodysplastic or myeloproliferative syndrome have a worse prognosis. The same applies to cases of AML associated with chemotherapeutic cancer treatments.
The patient’s physical condition and activity level also play a substantial role in the prognosis of AML. For example, patients that are older than 60 years of age and that possess high levels of lactate dehydrogenase have a significantly worse prognosis than younger patients.
Survival rates in most clinical trials hover somewhere between 20% and 50%. However, it is important to note that most clinical trials studying patients with AML focus on a younger demographic, who is much better suited to tolerate aggressive types of therapy. Therefore, it is very likely that the overall survival rate for all patients with AML, including the elderly and patients who are unable to tolerate aggressive types of therapy, is much lower.
Treatment of Acute Myeloid Leukemia (AML)

In some cases, the diagnosis of AML represents a very high number of leukemic cells in the patient’s blood, which can cause severe circulatory problems, along with a number of neurological symptoms and, in some cases, complete respiratory or even circulatory collapse.
As explained before, AML is a complex disease with different clinical forms and subtypes, which represent different prognoses and highly variable responses to treatment.
Therefore, the treatment options available to each patient are based on the identification of the specific leukemia subtype, which can be done through a number of laboratory tests, and the interpretation of the individual’s prognostic characteristics or factors.
Several types of treatment can be used to treat people with AML. However, all of them focus on the effective elimination of leukemia cells, damaging as little as possible the normal cells of the bone marrow and other tissues of the patient.
Some of the most common avenues of treatment include:
• Chemotherapy
• Bone Marrow Transplant
• Allogeneic Stem Cell Transplant