Our bodies were first thought to be hollow vessels in which our souls reside. The reality proved to be the complete opposite but nevertheless fascinating. Our body is formed by billions of cells working in perfect harmony that initially started from a single one. Our organs need oxygen to survive to produce energy, and the delivery of oxygen along with countless other nutrients and chemicals is carried out by blood. The blood is formed of a fluid component called plasma and a cellular component. Cells of the blood are unique and differ from each other in most of their properties and functions, and all of them originate from the bone marrow.
What is the bone marrow?


During fetal life, the blood is created in many organs including the liver, bones, lymph nodes and a vestigial structure called the yolk sac. When the baby is born, his or her blood is only formed in a group of stem cells in the cavities of bones called the bone marrow. Bones -especially long bones like the thigh- are composed of a hard shell called the cortex and a soft cavity within called the medulla. The medulla is filled with a soft tissue called the marrow. It is formed of cells that divide adequately to form all blood components. The main types of cells are the common myeloid progenitors, which give rise to red blood cells, platelets, and all white blood cells except for lymphocytes. The common lymphoid progenitor gives rise to lymphocytes. Other cells found in the bone marrow are fat cells, bone cells, and fibroblasts, which form the connective tissue framework that supports these cells.
The bone marrow is “red’ at birth, which means that it is very active that most of its cells are stem cells actively producing blood elements. As we age, most of these cells are replaced by fat cells “adipocytes,” and by adulthood, the red marrow is only found at the ends of long bones, the sternum, and the hip bone.
Bone marrow disorders


Even though the process of blood formation or “hematopoiesis” is very delicate and finely calibrated, since can go wrong for a multitude of reason because of the fact of the presence of stem cells. Stem cells can form virtually any cell and can be damaged easily. You can imagine them as a fragile marble block that can break easily with a wrong hammer stroke and has the potential to make any statue. Disorders of the bone marrow can be broadly classified as:
- Aplastic anemia
- Pancytopenia
- Malignancy
Since the bone marrow acts as a factory for the production of blood cells, the disorders are either due to decreased production -aplastic anemias if the product is red blood corpuscles and pancytopenia if all blood cells are affected- and cancers. Cancers that are found in the bone marrow can either be primary “leukemia” where they originated from the same cells of the bone marrow or secondaries “metastases” from other cancers that moved along the bloodstream and were dislodged in the bone marrow.
Aplastic anemia and pancytopenia


Aplastic anemia is the condition in which the bone marrow is no longer able to produce red corpuscles in sufficient amounts, and pancytopenia means that the bone marrow can no longer produce any cellular element in adequate amounts, be it red corpuscles, white cells or platelets.
Such a condition can result from a multitude of causes; however, in most cases, a definite cause cannot be established. They may result from viral infections, after chemotherapy or radiotherapy, or due to long-standing chronic debilitating diseases as cancer and liver failure. When patients present with aplastic anemias or pancytopenia, they exhibit features of deficiency of blood elements. For example, patients who have anemia suffer from easy fatiguability, breathlessness, effort intolerance and depressed brain functions. Patients who suffer from decreased white blood cell count suffer from repeated and non-resolving infections. They may also suffer from opportunistic infections, which are organisms that generally can’t infect healthy human beings but take advantage of the weakened immune system to produce severe infections, while patients with decreased platelet count suffer from easy bruising and bleeding which can occur from virtually all mucosal surfaces be it the mouth, the gastrointestinal system, the nose, the urinary tract or may even manifest as heavy menses in reproductive-age females.
Aplastic anemia is a potentially fatal condition unless adequately treated, and treatment is dependent on the cause, but if the cause cannot be specified or is treated and the bone marrow didn’t recover, bone marrow transplant remains the ultimate solution.
Malignancy (bone marrow cancer)

A common characteristic of cancers is that they originate from biologically immortal cells, and when such cells are stem cells with the potential to differentiate into many cells, the problem becomes more complicated. Bone marrow cancers are diverse and are divided into two main categories: primary bone cancers which originated in the bone marrow itself, and secondary cancers which originated elsewhere in the body and then traveled along the bloodstream to reach the bone marrow among other organs. By far, the metastatic bone marrow cancers are more common.
Primary bone cancers may either be leukemias or lymphomas. The main difference is that lymphomas don’t release cancerous cells in the blood, while leukemias do -although this definition became somehow obsolete in the last few years-. They manifest by a variety of symptoms which include general symptoms of malignancy as fever, night sweats, loss of weight with loss of appetite and enlarged lymph nodes. Other more specific symptoms of malignancy differ according to the type of leukemia and lymphoma.
Lymphoma of the bone marrow
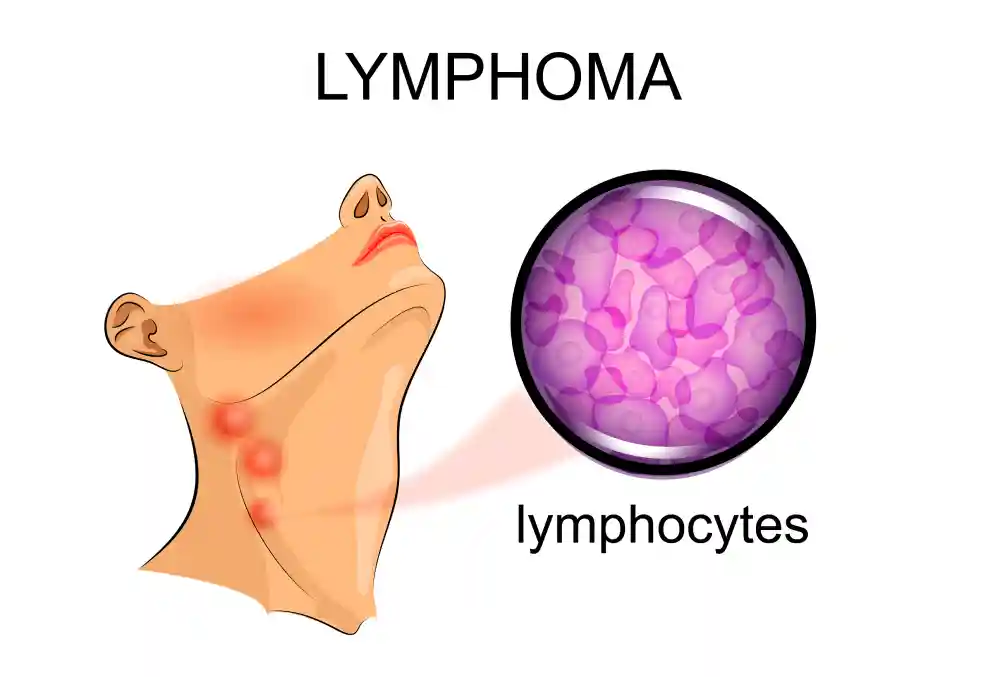

Lymphomas, in general, are classified into Hodgkin’s and Non-Hodgkin’s lymphomas, and the type of lymphoma that affects the bone marrow is almost always Non-Hodgkin’s lymphoma. Lymphomas originate from lymphocytes, which are white blood cells that are found in the lymph nodes, bone marrow, gastrointestinal system and many other areas. Many risk factors can cause Non-Hodgkin’s lymphoma including viruses as hepatitis C, human T-cell lymphoma virus and Epstein-Barr virus, autoimmune diseases as rheumatoid arthritis, systemic lupus and celiac disease, chemicals especially herbicides and pesticides, radiation exposure and some genetic conditions. Although lymphomas may be asymptomatic until late in the disease, enlargement of the lymph nodes with the associated symptoms of malignancy, especially bone pains or splenic enlargement, should alert the physician of suspected malignancy. Lymphomas are diagnosed classically with a lymph node biopsy from enlarged nodes and radiologic assessment of the disease using CT scanning or MRI. Treatment can be through chemotherapy, radiotherapy, immunotherapy or a combination.
Leukemia
Leukemia is a type of cancer that affect stem cells in the bone marrow, causing the affection of all blood elements. Leukemias are divided into acute and chronic leukemias and each one is divided into myeloid and lymphoid. The main difference between acute and chronic leukemias is the type of cells affected, the presence and severity of symptoms and therefore, the treatment given.
Chronic leukemia
Chronic leukemias manifest by the rapid division of elements of the bone marrow. It results from the genetic mutation called the Philadelphia chromosome, where 2 chromosomes break at different points and exchange their genetic material producing a deformed protein called tyrosine kinase. They are divided into chronic myeloid and lymphoid leukemias:
- Chronic myeloid leukemia: They are chronic leukemias that originate from the myeloid components of the bone marrow, which are the red corpuscles, all white cells except for lymphocytes and platelets. The condition may be asymptomatic, but it chiefly presents by an enlarged spleen which may or may not be associated with the general symptoms of cancer. Chronic myeloid leukemia may also present paradoxically with increased bleeding tendency even though the platelet count is high. This is because the formed platelets are non-functional. Chronic myeloid leukemia is treated by a novel class of drugs called tyrosine kinase inhibitors which act not only to decrease the cell count but on a genetic level to repair the primary defect that caused leukemia to develop in the first place.
- Chronic lymphoid leukemia: Chronic lymphoid leukemias are not so different from their myeloid sisters, except that they originate from the lymphocytes and that they are less commonly symptomatic. Unlike myeloid leukemias, they have a strong causative relationship with chemical exposure, especially pesticides, and that’s why they are commonly encountered in farmers. They are treated more conservatively with watchful waiting as they develop in older age groups “above 60” and are less prone to complications. Treatment options are quite limited including chemotherapy, radiation therapy and bone marrow transplant.
Acute leukemia
Acute leukemia is quite different from chronic leukemia in that they are symptomatic from the start with severe manifestations of malignancy, as mentioned above. Bone pain is evident and can be the presenting symptom. Due to the malignant invasion of the bone marrow by blast cells, almost all blood elements are defective, and the patient may present with severe anemia. Acute leukemias develop because the stem cells of the bone marrow “arrest” and don’t continue the normal pathway of development, producing the characteristic dysfunctional cells. Acute leukemias are divided into:
- Acute myeloblastic leukemia: Acute leukemia has many risk factors, including other hematological diseases as primary myelofibrosis and aplastic anemia, congenital disorders as Down syndrome and exposure to radiation or chemotherapeutic agents. AML presents with the deficiency of all blood elements due to the replacement of the healthy marrow with the immature cells. Therefore, it causes severe anemia, immunodeficiency and bleeding due to platelet deficiency. Acute myeloid leukemia is treated by a combination of chemo and radiotherapy.
- Acute lymphoblastic leukemia: It is similar to myeloid leukemia in most symptoms although it is less likely to develop severe anemia due to the proliferation of lymphoblasts “the immature cells,” they invade other structures as the lymph nodes, spleen and liver causing their enlargement. Acute lymphoblastic leukemia is treated by chemotherapy with special care for the brain and the central nervous system whether surgical, radiotherapy or chemotherapy explicitly designed for its treatment.
Blast crisis
Chronic leukemias, especially chronic myeloid leukemia have a mild course of action for the first few months to years. However, as time passes the risk of development of what is called a blast crisis increases. Blast crisis is when the count of blast cells increases to 20% of all white blood cells, while the normal count in the blood of a chronic leukemia patient rarely exceeds 5%. The dangerous consequence of such rapid proliferation of cells is that it develops a condition known as leukostasis when the count of cells exceeds 500,000 per cubic milliliters, which produces symptoms and complication similar to blood clots as breathlessness, strokes and transient ischemic attacks -reversible “mini-strokes” of the brain- and priapism – prolonged unexplained penile erection which can compromise its blood supply-. Blast crisis needs immediate combination radiotherapy and chemotherapy, the same as acute leukemia, but with a worse prognosis.
Bone marrow biopsy
One of the most frequent hematological investigations ordered in leukemia is a bone marrow biopsy. Since bone marrow is the leading manufacturing plant of blood cells, and since it is hidden under a layer of thick bone, we need special techniques to obtain a sample for investigations. After birth, and as the human advances in age, the percentage of the active “red” marrow decreases. By late childhood and early adulthood, it becomes almost entirely replaced by the inactive “yellow” marrow, and the active marrow becomes limited to the axial bones especially the sternum, ribs, hip bone and the proximal ends of long bones -the parts near the center of the body-.
Bone marrow biopsy is ordered for the following conditions:
- Unexplained anemia decreased platelets or even increased white blood cells.
- The diagnosis, staging, and monitoring of the treatment of hematological malignancies whether leukemias, myelodysplastic disorders, lymphomas or multiple myeloma.
- Fever of an unknown origin.
- Some rare metabolic diseases as Nieman-Pick and Gaucher.
- Metastatic cancers from elsewhere in the body and staging of other granulomatous diseases as sarcoidosis and tuberculosis.
There are two main types of bone marrow biopsy: aspiration and trephine biopsy. In bone marrow aspiration, the doctor will push a needle through the thick bone -under local anesthesia- and then aspirate a small amount of the marrow. This procedure is used in case of some bone cancers to get a general look at the cellular components of the bone marrow. Trephine bone marrow biopsy, on the other hand, involves the sampling of a small part of the cortical bone with the marrow underneath with a special needle and technique. It is more accurate than bone marrow biopsy and is the only option in cases where bone marrow aspiration cannot be done as in cases of aplastic anemia and metastatic cancers.
Bone marrow biopsy results

After the biopsy specimen or aspirate is sent to the lab, results come out:
- To confirm or contradict the diagnosis.
- Stage the disease
- Show response to treatment.
Biopsy results mainly involve the following categories:
- Cellularity: This is a general look on the number of cells in the bone marrow, a hypercellular bone marrow can be an indication of cancer or increased peripheral destruction of blood cells necessitating increased production as in cases of hypersplenism -a condition which involves an enlarged spleen that excessively destroys blood cells-, while a hypocellular bone marrow can be seen in aplastic anemia or bone marrow failure.
- Cellular components: This is a specified view on the bone marrow, and its different cells, the presence of blast cells is normal in the bone marrow as long as they don’t exceed 20%. Otherwise, it is a sure diagnosis of acute leukemia.
- Abnormal components: Some components of a bone marrow biopsy are abnormal, and shouldn’t be there. For example, in hemochromatosis, where excessive iron is deposited in the marrow, or Gaucher and Niemann-Pick diseases, in which excessive fat is found. Another example is amyloidosis, in which excessive amounts of an abnormal protein called amyloid are deposited in the bone marrow.
- Immunophenotyping: This type of investigation is directed towards the identification of the source of malignant cells. Bone marrow cancers as leukemia are known to be monoclonal, which means that they originated from a single mother cell, and proving this relationship is enough to both diagnose cancer and to diagnose this leukemia as myeloid or lymphoid.
Bone marrow transplantation

Blood cells originate from a cell in the bone marrow called the hematopoietic stem cell. It has the potential to differentiate into all the blood cells that originate in the bone marrow, and when these stem cells are destroyed beyond a certain point, they cannot regenerate, and the production of blood cells is impaired. Bone marrow transplantation involves obtaining such cells from another person -and sometimes the same person before starting a treatment for another condition that will potentially or inevitably destroy the bone marrow-, processing them and then infusing them through a catheter. Bone marrow stem cells can be obtained from the bone marrow itself, from peripheral blood just like a normal blood sample or umbilical cord blood -although the latter 2 methods yield less and are not suitable for all cases-.
Bone marrow transplantation is used in the following conditions:
- Hereditary diseases when either red cell production or immunity are severely impaired.
- Some red cell disorders as Thalassemia and sickle cell anemia.
- Immunodeficiency disorders, especially AIDS.
- Malignancy and premalignant conditions of the bone marrow.
- Bone marrow failure and aplastic anemia.
The procedure


Bone marrow transplantation involves the following steps:
- Finding a suitable donor: Bone marrow is an organ, and any organ that is transplanted carries the risk of rejection, but consider this: When an organ is rejected, it is the immunity of the body that refuses its presence and considers it a foreigner, but what if the immunity itself is transplanted and considers the whole body a foreigner? This is the case in bone marrow transplantation, and that’s why many tests are carried out to ensure the suitability of the donor. The perfect donor is always the same person or an identical twin, followed by a first-degree relative.
- Conditioning: This process involves different steps of preparing the body to receive the bone marrow, the present marrow is ablated using chemotherapy and radiotherapy, to make space for the new marrow.
- Infusion: Infusion of the new marrow is carried out through a central venous catheter -in the neck veins for example- over a period of one hour or more.
After the previous procedures, the body becomes severely immunodeficient “the neutropenic phase,” since the bone marrow transplanted needs time to develop immunity after the destruction of the old one. During this period, the patient undergoes isolation to protect him from catching any infection, and antibiotics and antifungals are given even without an identifiable infection. After about 4 weeks, symptoms of immunodeficiency subside and the patient is put under observation until discharge.
Bone marrow transplantation risks

Although bone marrow transplantation is sometimes the only available option, risks have to be considered, and patients informed about the known complications of marrow transplantation. The most common problems include:
- Severe infections: Patients during the immunodeficiency phase have a nonexistent immune system and could easily develop severe infections; most of them are not even possible in healthy individuals, the so-called opportunistic infections. The sources of infections are various, but the most serious of which are the hospital-acquired ones, since they are resistant to antibiotics and are therefore difficult to treat.
- Cancers: Although bone marrow cancer may be an indication of bone marrow transplantation, other cancers may develop from the radiation used for destroying the old marrow.
- Graft versus host disease: This is a rejection process of the newly transplanted marrow. As mentioned above, here the marrow rejects the whole body rather than vice versa which necessitates immunosuppressive therapy and could cause severe immunodeficiency.
Bone marrow donation


Since the bone marrow is an organ, and since it is sometimes considered the only definitive treatment in many conditions, bone marrow donation is an integral part of any healthcare system. All body organs are “coded” with receptors on the surface of their cells which serve as an ID to tell the immune system that they belong to the same body. They are called MHC or “Major Histocompatibility complexes.” When transplanting an organ, we have to make sure that both the transplanted organ and the body are compatible to prevent the development of graft versus host reaction or “rejection.” Therefore, transplanted organs from the body itself or an identical twin are unparalleled and need no special measures for immunosuppression, followed by those from close family. Stem cells can be taken both from the bone marrow itself or the peripheral blood.
Bone marrow donation risks

Bone marrow donation is a relatively safe procedure and carries no risks other than those related to the setting of the procedure itself. In case of bone marrow donation from the marrow itself, the main risk is that of the anesthesia and the small wound found at the back of your pelvis no more than a centimeter across. Peripheral bone marrow donation is much safer and carries minimal risks, but the choice of the type of donation depends on the amount needed and the resources available at the hospital to obtain enough blood stem cells from the peripheral blood.