What is chronic lymphocytic leukemia?


It is known either as chronic lymphocytic leukemia or as chronic lymphoid leukemia, and it is a blood cell disorder and a type of blood cancer. Chronic lymphocytic leukemia features an accumulation of lymphocytes in the blood that are incompetent and not completely functional. It is the most common type of leukemia in adults living in Western countries, and even though the majority of patients survive, some of them may die due to complications we will explain further.
This disease is more common in white males and the elderly, and less common in African Americans and females. According to the American Cancer Society, there were near 21,000 new cases of chronic lymphocytic leukemia in 2019, in the United States alone. This is an estimate, and the true incidence is apparently higher because many new cases are not diagnosed or reported. Other countries in the Western world have a similar incidence, but the disease is very rare in Japan, China, and other Asian countries.
What causes chronic lymphocytic leukemia?


Similar to many other types of cancer, chronic lymphocytic leukemia does not have a single cause. It is a multifactorial disease, which means that many different causes interact with each other. There is not an exact cause already identified, but we do know that genetic factors are not as prevalent as in other diseases. It is an acquired disorder, and the majority of cases do not have a familial medical history. In rare familial cases, the median age is reduced from 72 years to 58 years old.
The majority of genes that cause chronic lymphocytic leukemia are proximal to genes that regulate apoptosis. The most common genetic abnormality is a deletion of gene 13q14, and it happens in around half of these patients. When they have this abnormality, their disease progresses very slowly and it is relatively stable. Another abnormality is a trisomy of chromosome 12, which appears in around 15% of patients and 17p13 gene deletions, which compromise the normal function of the p53 tumor suppressor gene. Additionally, it is very common to have an overexpression of a gene called bcl2. This is a proto-oncogene, which means it is a normal gene that triggers cancer when overexpressed.
As a result of a series of genetic alterations in monoclonal cells, patients with chronic lymphocytic leukemia become arrested in the differentiation pathway. The type of cells involved are B-cells, which stays as pre-B cells and do not reach the mature B cell phase. Still, in blood tests, they resemble mature cells very closely, and that’s why they are often counted as such.
Chronic lymphocytic leukemia symptoms
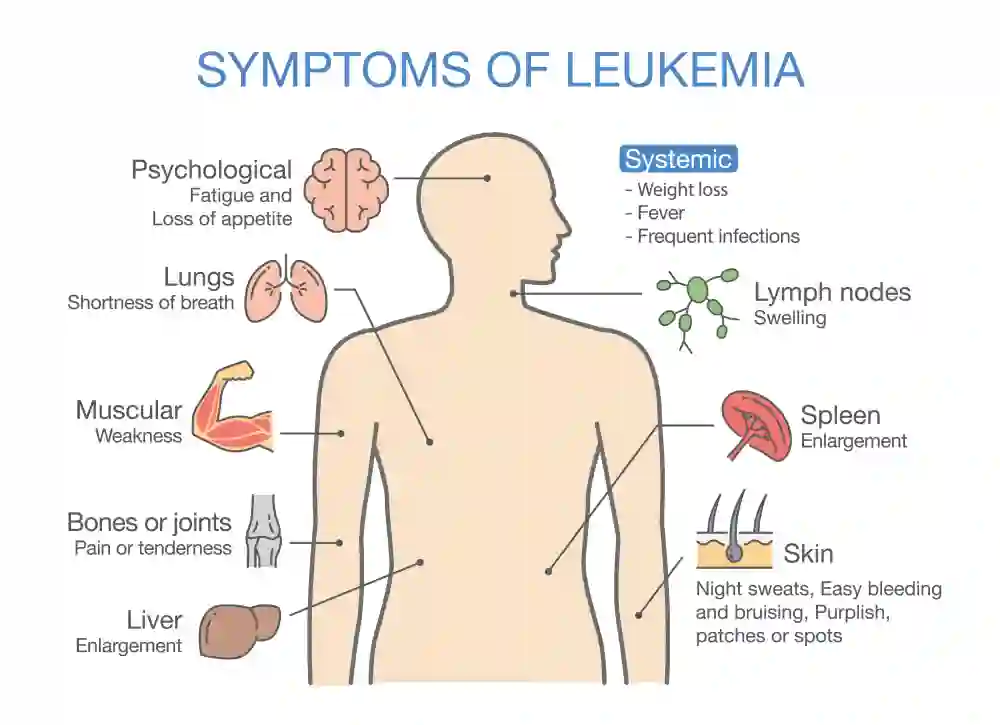

Patients are usually diagnosed with chronic lymphocytic leukemia when the disease has already established for a few years. In up to 50% of cases, it is asymptomatic at the moment of presentation, which means it does not give out many signs and symptoms. After an insidious onset, patients are usually diagnosed after a routine blood cell count. During a progressive disease, and in symptomatic phases, the most common signs and symptoms are as follows:
1. Enlarged lymph nodes


It is the most common symptom, which is found in almost 90% of patients. It is because the disease is located in the immune system cells, and the lymph nodes are important in storing this type of cell.
2. Predisposition to infections


There is excess lymphocytes in chronic lymphocytic leukemia, but they are immature and not functioning properly. Thus, patients present with repeated infections, especially viral infections such as herpes zoster, herpes simplex, and viral pneumonia.
3. Fever, chills, and night sweats


As a result of recurrent infections and immune system dysfunction, patients start experiencing an increase in body temperature. Chills and night sweats are attempts of the body to increase body temperature by a transformation of mechanical energy into heat.
4. Petechiae and mucocutaneous bleeding


Many patients with chronic lymphocytic leukemia develop thrombocytopenia as well. This is because excess lymphocytes start occupying the place reserved to other blood cell types, and patients end up with mucocutaneous bleeding and skin rashes.
Read Also; How to Increase a Low Platelet Count!
5. Fatigue

Tiredness and fatigue are common, especially in patients with anemia. This condition often develops for the same reasons as thrombocytopenia.
6. Pallor


Another sign of anemia is pallor or pale skin. This is because the color of the blood is less intense, and the circulation of blood becomes affected by the disease.
7. Enlarged spleen and liver


The spleen and liver are always in contact with the blood, and they become infiltrated by aberrant cells. The most common organ enlargement is splenomegaly, which can be found in more than 50% of cases, and hepatomegaly appears in up to 20% of cases.
8. Weight loss

It is a common feature in the majority of cancers, including blood cancer. Weight loss often appears in a late stage of the disease, and it is a part of a wasting syndrome called cachexia, which includes poor appetite, weight loss, and fatigue.
Chronic lymphocytic leukemia diagnosis


The most important part of the diagnosis in chronic lymphocytic leukemia is a complete blood cell count. In some cases, it is the only way to diagnose the disease because patients are asymptomatic and the discovery is nothing but casual. Tests will show lymphocytosis, and blood cell count usually reaches 5000 B-lymphocytes per microliter or more. The diagnosis is made by looking at the signs and symptoms and performing another test after 3 months, which shows the same type of lymphocytosis.
In some cases, patients have fewer than 5000 B-lymphocytes per microliter with swollen lymph nodes, and differential diagnosis should be made with small lymphocytic lymphoma. In these cases, it is necessary to confirm the diagnosis through a lymph node biopsy.
It is also important to perform a microscopic examination of the peripheral blood to confirm lymphocytosis. There will be around 50% of large and cleaved lymphocytes, but more than that is usually due to another type of leukemia, called prolymphocytic leukemia.
Other tests such as flow cytometry should be done to confirm clonality. It is useful to check the presence of surface proteins such as CD20, CD23, CD5, and CD19.
In patients with recurrent infections, it will be necessary to perform immunoglobulin tests and consider the administration of monthly immunoglobulin in patients with lower than 500 mg of IgG.
Another differential diagnosis includes hairy cell leukemia. This type of leukemia has positive surface immunoglobulin, and it is negative for certain surface proteins, including CD21 and CD5.
It may be necessary to perform a bone marrow aspiration, especially when trying to diagnose complicated cases of chronic lymphocytic leukemia. In the majority of cases, it is not required. Other tests usually performed in the diagnostic phase and later on include an abdominal ultrasound to detect liver or spleen enlargement.
Chronic lymphocytic leukemia prognosis


The majority of patients with chronic lymphocytic leukemia live for 5-10 years or more because this is a slowly progressing disease and relatively benign. Patients who die from chronic lymphocytic leukemia usually go through a terminal phase that is more rapidly progressive and lasts for 1 or 2 years. In other cases, patients develop complications and these may be as severe as to cause their death 2 or 3 years after diagnosis.
Still, the prognosis of chronic lymphocytic leukemia widely depends on the stage of the disease at the moment of diagnosis, the presence of certain risk markers and complications at some point of the disease.
The most common complications are:
• Infections: They are caused by a weakened immune system. What is usually a mild or harmless infection in normal patients may become severe and life-threatening in patients with lymphocytic leukemia.
• Ritcher’s syndrome: In some cases, chronic lymphocytic leukemia turns into lymphoma, and this transformation is named Ritcher’s syndrome. It is an aggressive complication that should be treated promptly with chemotherapy and other medications.
• Autoimmune hemolytic anemia: The immune dysfunction in chronic lymphocytic anemia may lead to autoimmune conditions. In autoimmune hemolytic anemia, the immune system attacks red blood cells and destroys them. It results in severe anemia that is treated with steroids and other medications.
Chronic lymphocytic leukemia treatment

Treatment for chronic lymphocytic leukemia is not required unless patients have symptoms such as extreme fatigue, weight loss of 10% or more over the last 6 months, fever for 2 weeks or more, massive lymphadenopathies, autoimmune anemia, thrombocytopenia that does not respond to steroids, and progressive lymphocytosis of 50% in two months.
When necessary, treatment includes chemotherapy that combines alkylating agents, nucleoside analogs, and biologic agents. The only way to cure the disease is through allogeneic stem cell transplantation, and remission of the disease is defined by a total absence of lymphadenopathy, lymphocytosis, and organ enlargement.
References
Nabhan, C., & Rosen, S. T. (2014). Chronic lymphocytic leukemia: a clinical review. Jama, 312(21), 2265-2276.
Slager, S. L., & Kay, N. E. (2009). Familial chronic lymphocytic leukemia: what does it mean to me?. Clinical Lymphoma and Myeloma, 9, S194-S197.
Hallek, M., Cheson, B. D., Catovsky, D., Caligaris-Cappio, F., Dighiero, G., Döhner, H., … & Kipps, T. J. (2008). Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute–Working Group 1996 guidelines. Blood, The Journal of the American Society of Hematology, 111(12), 5446-5456.
Wang, L., Lawrence, M. S., Wan, Y., Stojanov, P., Sougnez, C., Stevenson, K., … & Zhang, W. (2011). SF3B1 and other novel cancer genes in chronic lymphocytic leukemia. New England Journal of Medicine, 365(26), 2497-2506.