
Acute leukemia has 2 subtypes. They are acute myeloid leukemia, and acute lymphoblastic leukemia and their diagnosis depend on the cells involved, and the progression of the disease. Acute myeloid leukemia can further be subdivided into further 8 subtypes, depending on the maturity of the cells that are proliferating in the bone marrow. They are range between M0 through M7 according to the differentiation of cells. Another way to classify AML is through the genetic alterations that occur in patients, which is the current classification by the World Health Organization. Similarly, an acute lymphoblastic type has 4 types depending on the cell involved in the lymphoid series. The types include B cell ALL, T-cell ALL, and an undifferentiated type.
Similar to acute leukemia, chronic leukemia also has been divided into chronic myeloid and chronic lymphoblastic types and subtypes. Chronic lymphoblastic types include common B cell and Rare T cell CLL. On the other hand, chronic myeloid leukemia has 4 types depending on the presence and absence of the Philadelphia chromosome and the BCR gene.
But, with so many options, types, and subtypes, how can we diagnose them?
How is leukemia diagnosed?


Every ailment manifests with different signs and symptoms depending on the duration and nature of the disease. These clinical features help in making a diagnosis or suspecting the nature of a given disease. However, confirmation is always required to make a diagnosis. This can be achieved by doing various blood tests, radiographic investigations, and cultures.
Clinical features to suspect leukemia include a fever of unknown origin, tiredness, shortness of breath, abdominal discomfort and pain, anorexia, sweating, bone pain, recurrent infections, and easy bruising. Other signs and symptoms include enlarged lymph nodes, pallor, oral thrush, and petechial rashes on the body.
The age group is another important factor in determining the type of leukemia. For instance, AML is common in the pediatric age group and ALL in adults. CML is more common in ages above 50 years, and CLL is usually seen above 65 years old.
Another clue that leads to diagnosis is where people work and their health risks. For example, industrial workers who get exposed to benzene have a higher chance of suffering from leukemia. The same goes for people working in radiology departments or hospitals. We can see leukemia more commonly in whites as compared to other races, and it is more common in patients with a positive family history, identical twins, and immunocompromised individuals. These factors help doctors suspect leukemia and make the appropriate tests for diagnosis.
Once these factors are taken into account, the next thing would be performing a physical examination of the patient. In examining the body, doctors will usually look for pallor, a lethargic look of the patient, bruises on the body, an enlarged and tender abdomen, enlarged lymph nodes, rumbling murmurs at auscultation, and many other leading signs. If there is an active infection, doctors will be able to detect them in some cases, and depending on the signs and symptoms the patient has. After this, confirmatory tests are carried out to make sure if it is leukemia or any other disease process.
For each type of leukemia, there is a protocol designed to diagnose patients. For example:
Acute myeloid leukemia


In this type of leukemia, one of the most important exams for diagnosis is blood tests. Doctors can also order diagnostic imaging tests and a bone marrow aspiration with biopsies, which is the definite diagnostic test. Additionally, it is possible to analyze the predominant genetic abnormalities, which help in classifying acute myeloid leukemia. All of these exams give doctors prognostic information, and they guide the treatment of the condition at all stages of the disease. After treatment is started, it is common to perform additional tests to evaluate cardiac function because most chemotherapeutic agents are cardiotoxic.
Acute lymphoid leukemia


In acute myeloid leukemia, more tests are usually required. Blood tests should be accompanied by a peripheral smear, and doctors typically ask for liver and renal function tests. Blood cultures are sometimes required, depending on the signs and symptoms of the patient, and imaging studies are also useful, especially in cases of infection. Doctors can order a lumbar puncture, an echocardiogram, and other types of specialized tests. However, the definite diagnostic test is the same: a bone marrow aspiration with a biopsy. For classification, it will be important to detect genetic abnormalities in the bone marrow and the lymphoblasts in the peripheral blood. All of this is useful for prognosis, too, and can be ordered more than once, depending on the signs and symptoms of the patients.
Chronic myeloid leukemia

It is often detected accidentally when doctors order a complete blood test to detect other ailments. However, lymphocytosis in the complete blood counts must persist for at least 3 months to make the diagnosis of chronic myeloid leukemia. Other tests should be performed as well, including a peripheral blood smear and flow cytometry. In some cases, the differential diagnosis with small lymphocytic lymphoma should me bade. In these cases, it will be necessary to perform a biopsy of the lymph nodes. In patients with repeated infections, it will be useful to get their quantitative levels of immunoglobulin to plan ahead for the treatment.
Chronic lymphoid leukemia


Similar to chronic myeloid leukemia, CLL is also diagnosed through a complete blood test, which is usually performed to detect other diseases. To fully diagnose the disease, it must be associated with persistent changes in the blood count values, and doctors should order a peripheral blood smear. Imaging studies are useful to detect splenomegaly and hepatomegaly, but they are usually very large and determined by physical examination only. Different from other types of leukemia, the diagnosis of chronic lymphoid leukemia is based on finding the Philadephia chromosome in the cells of the bone marrow. Thus, it requires a histopathologic and genetic analysis of the bone marrow and the peripheral blood. Other tests that may be useful depending on each patient include blood chemistry and specific tests and cultures in infected patients.
Leukemia blood tests

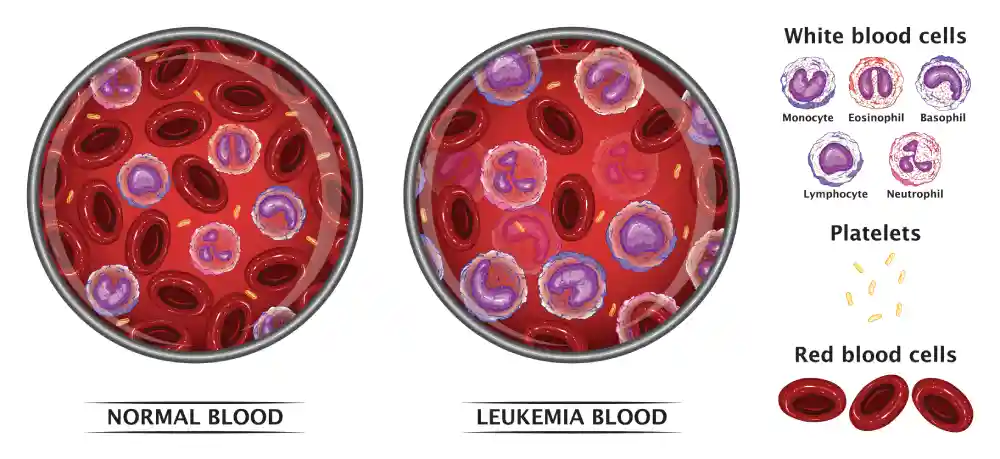
As discussed earlier, in leukemia there is an abnormal proliferation of white cells in the bone marrow which spill into the bloodstream and cause various complications. Therefore, it is important to identify abnormal values in the blood and in key organs of the body, such as the liver, heart, bone, and lungs. The blood tests include:
- Coagulation Profile: tests include Prothrombin Time (PT), which determines if there is any defect in the extrinsic pathway in the coagulation cascade. APTT (Active ThromboPlastin Time) is another test that can be deranged when there is a defect in the intrinsic pathway of the coagulation cascade.
- Renal function tests: Include the creatinine and urea levels, which get deranged in patients with acute infection.
- Liver function tests: Serum Alkaline Phosphatase, AST, and ALT levels are deranged in leukemic patients, and they show that the liver is not functioning properly.
- Complete Blood Count (CBC): The white cell count gets higher than normal, sometimes alarmingly high. CBC is the first test every doctor looks at because they are quite common for most diseases. Decreased Hemoglobin and decrease in platelet count are common findings in leukemic patients, too.
- Serum Electrolytes: As the patient cannot get proper blood supply to the tissues, the body gets weak. This is apparent in serum electrolyte analysis, which shows abnormal levels of sodium, potassium, and calcium.
- Bone marrow aspiration/Biopsy: It is not a blood test, but should be highlighted because it is an important diagnostic test, which determines the cause of leukemia and the type of leukemia present. Bone marrow aspiration or biopsy is often the definite diagnostic test for leukemia.
Leukemia prognosis

There are many prognostic factors for leukemia patients:
- Age: Survival rate depends on the age of the patient, sometimes. However, this is not the same for all types of leukemia. In most cases, the extremes of life are associated with more aggressive leukemia types.
- Leukocyte count: Increased WBCs lead to poor prognosis in leukemic patients.
- Presence of blasts in peripheral smear: As the number of immature blood cells increases in the peripheral blood, the prognosis of the patient will be worse.
- Time of Diagnosis: An early diagnosis leads to early treatment and increases the chances of survival.
References
Haferlach, T., Kohlmann, A., Schnittger, S., Dugas, M., Hiddemann, W., Kern, W., & Schoch, C. (2005). Global approach to the diagnosis of leukemia using gene expression profiling. Blood, 106(4), 1189-1198.
Katz, R. L. (1991). Cytologic diagnosis of leukemia and lymphoma. Values and limitations. Clinics in laboratory medicine, 11(2), 469-499.
Cortes, J., & Deininger, M. (Eds.). (2006). Chronic myeloid leukemia. CRC Press.
Reaman, G. H., & Smith, F. O. (2014). Childhood leukemia. Springer.