Ever since we were born, very few of our cells remained the same, and they are mostly neurons (nerve cells). Otherwise, the rest of the cells are in a continuous state of death and division. This has to be tightly controlled to avoid decreased or increased number of cells in a given tissue, and those control mechanisms are also dependent on the state of the body and its need for new cells of a specific type. This is what makes the human body so complex.
The main key to such complexity is our DNA, the blueprint of our bodies. If our DNA is altered, and several repair mechanisms fail to fix the defect, our cell also has other self-destruct mechanisms to avoid harm. If all the previous defense mechanisms fail at the same time, cancers can develop.
What is the bone marrow?


If our blood cells were to be manufactured products, the bone marrow would be the manufacturing plant, and raw materials are called stem cells. These stem cells differentiate into the different cells floating in our blood stream, namely red blood cells -or corpuscles to be more precise-, white blood cells and platelets.
The bone marrow is located within the cavities of long bones as those of your thighs and arms as well as bones of the axial skeleton including the ribs, skull and the hip bones. If you ever tasted or saw marrow of cattle, you’ll notice that it is very greasy and mainly has fat in it. That is because starting from childhood and until adulthood, the red bone marrow is replaced by fat cells, and by late adulthood the active or red marrow is only found in the thighs, hip bone and perhaps the breastbone, or “sternum”.
How does polycythemia develop?
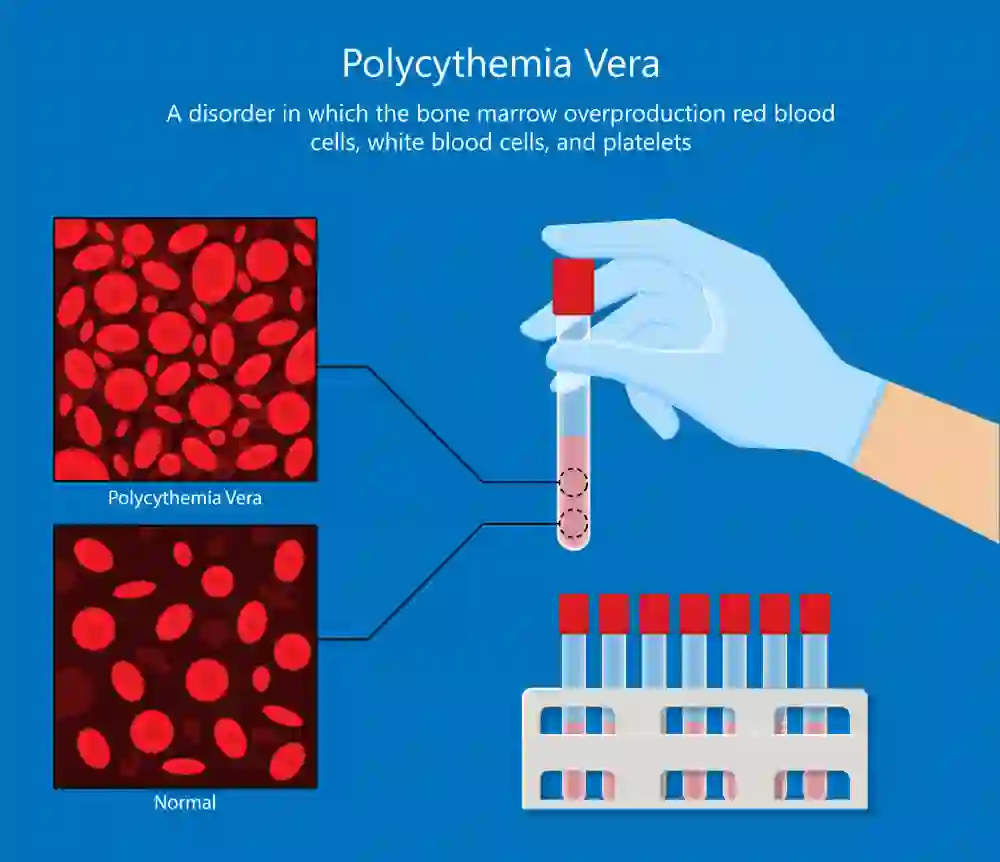

Before describing how polycythemia develops, we have to understand that this isn’t the only type of polycythemia and the term polycythemia means an increase in red blood cells. Polycythemia is classified into primary and secondary, with polycythemia vera referring to the primary type. Secondary polycythemia is a physiological response to inadequate oxygen delivery to cells of the body, prompting the body to respond by increasing the rate of production of red blood cells. This usually occurs in people living at high altitudes or smokers and those with some lung conditions like chronic obstructive pulmonary disease (COPD).
Primary polycythemia belongs to a group of diseases called myeloproliferative neoplasms (MPN). Other members of the group include chronic myeloid leukemia, essential thrombocythemia and myelofibrosis. The common mechanism of such diseases is that they develop due to a genetic defect called a mutation that affects the signal pathway which usually controls the rate of division of such cells leading to uncontrolled proliferation, thereby the suffix “proliferative”. This mutation has been found in a gene called Janus Kinase or JAK-2 gene in more than 95% of cases. The same mutation has been also found in essential thrombocythemia and myelofibrosis indicating the genetic constituent of all myeloproliferative neoplasms.
Cancers develop due to mutations, and those mutations have several risk factors. In general, exposure to radiation or chemotherapy as well as heredity can play a role, but generally speaking, they are more common in the older age group starting from the 6th decade for some cancers like colon cancer, and the 7th decade in the case of blood malignancies. The idea behind that is the long series of divisions that those cells underwent, with the risk of an uncorrected mutation increasing as the time passes. This is the same reason as to why elderly mothers and fathers tend to have children with a higher risk of genetic mutations like Down syndrome. The longer a machine operates, the greater the risk it will make mistakes.
What happens in polycythemia vera?


Genetic mutations cause uncontrolled division of red cell precursors, as well as white blood cells and platelets. This is called trilineage proliferation with erythrocytic dominance, which means that the greatest difference in cell count is that of red cells.
This increased count causes an increased viscosity of the blood, which is responsible for most symptoms. Other symptoms result from the imbalance in the blood clotting mechanisms either due to increased platelet and red cell count or platelet dysfunction. Red cells are responsible for oxygen delivery through acting as carriers using the iron in hemoglobin, but an increase in their count can paradoxically impair such function due to the sluggish circulation of the viscid blood.
Polycythemia vera symptoms


Most symptoms of polycythemia result from the increased blood viscosity and tend to disappear when the hypercellularity is managed. They include:
1) Headache, dizziness, vertigo and tinnitus


They are nervous symptoms due to decreased oxygen delivery to the brain and the ears. Tinnitus is a buzzing sound in your ears that doesn’t stop and can vary from being unnoticeable to causing severe discomfort.
2) Weakness and fatigue

Our body needs oxygen in a steady supply to produce energy, and any inadequacy will cause our body to starve for energy, therefore we feel fatigue when such a capacity is reached. Fatigue is a common complaint of many conditions and can be overlooked by many physicians, but a careful history taking can prove crucial to determine the origin of the problem.
3) Chest pain

Symptoms of chest pain can be similar to heart attacks in polycythemia. If the blood can’t deliver enough oxygen to the tireless heart muscle, anginal pain develops. The only difference here is that the coronary arteries supplying the heart may be intact unlike the regular stable angina. The pain is usually felt like tightness either behind your breastbone at the middle of your chest or a choking sensation. In rare cases, it may be a sharp stabbing pain. It can also be felt in the left arm or neck. This pain characteristically worsens on effort and improves on rest.
4) Visual problems


The spectrum of visual disturbance due to hyper-viscosity of the blood is massive and ranges from blurring of vision to total blindness. Our retina is the main site for receiving visual signals, and it is highly susceptible to decreased oxygen levels, be it from a blood clot or from reduced delivery due to sluggish blood flow. The damage is usually reversible, but in prolonged conditions, visual loss can be permanent. Careful fundoscopic examination of the retina can lead the physician to suspect hyperviscosity.
5) Calf pain


One of the common complaints of those with problems with their peripheral blood vessels is intermittent claudication. A characteristic cramping pain of the calf muscles occurs on walking long distances due to the inability of such muscles to receive adequate blood supply to wash off the lactic acid that accumulated from their metabolism. Due to the sluggish blood flow, this can also occur in polycythemia. Pain tends to be relieved by rest.
6) Transient ischemic attack


Transient ischemic attacks are due to a small clot forming in the blood vessels supplying the nervous system but they usually resolve within the first 24 hours. Those symptoms include weakness of one side of the body, transient loss of sight in one eye, squint and double vision if the nerves supplying the eye are affected or numbness in the tongue or cheeks. This results from both the hyper-viscosity of the blood as well as the defective clotting mechanism that causes increased clot formation.
7) Abdominal pain

Due to the high turnover of cells in polycythemia, a large amount of chemicals is released from such cells including histamine. Histamine has a central role in immunity, but also acts to increase gastric acid production. If this occurs in excess, it can lead to gastric or duodenal ulcers producing abdominal pain which is usually located in the upper abdomen, burning in sensation and increased after meals.
Polycythemia vera diagnosis


Your doctor will perform a full physical examination with special emphasis on signs of blood disorders. A peculiar feature of polycythemia is a red plethoric face, this is owing to the increase in red cell count. This can also be noticed in the nails. Since the blood is thick and viscid, patients usually have hypertension. Other signs of blood clotting disorders can be seen including bruises and small red dots of the skin due to bleeding into the skin layers.
A) Laboratory investigations:


In all blood disorders, complete blood count constitutes the main laboratory investigation ordered, and PV is no exception. However, estimation of hemoglobin level or red cell count may be inaccurate since it is highly dependent on the plasma volume. For example: if there is severe dehydration or any other cause for loss of plasma fluids, the level of hemoglobin will be relatively increased and the same happens with blood viscosity. To overcome that obstacle, doctors use red cell mass measurement which involves the use of radioactive labeling of red cells. This is especially beneficial in cases when the hemoglobin level is between 16 and 20 g/dL.
Platelets and white blood cell count are also elevated. This is not very useful in the diagnosis of polycythemia itself but can be indicative of the risk of bleeding disorders.
Uric acid level is usually elevated due to the rapid turnover of cells, especially white blood cells. It is the product of cellular destruction and released in excess in cancers and other proliferative conditions since those cells tend to have a shortened lifespan. Uric acid crystals precipitate in the joints producing inflammatory pain and they are excreted by the kidney increasing the risk of urinary stones.
Reduced erythropoietin level: Erythropoietin is a hormone released by the kidney and functions to stimulate the bone marrow to produce more red cells. It is under the control of a feedback mechanism relating to the degree of blood oxygen concentration. Due to the increased red cell mass in polycythemia, the release of erythropoietin is suppressed. Renal functions should be assessed to make sure that this reduction is not due to a kidney problem.
Genetic testing: As mentioned before, the vast majority of polycythemia patients have JAK2 mutation. It is considered the backbone of polycythemia diagnosis.
Bone marrow biopsy: This isn’t a required test to diagnose polycythemia but can confirm the diagnosis and is considered a major criterion in the WHO diagnostic criteria of the disease. Findings will include a bone marrow with increased cellular component of the red cells, white cells and platelets.
To accurately diagnose polycythemia, doctors follow criteria established by the WHO in 2016 which are divided into major and minor ones.
- Major criteria include:
- Hemoglobin level of more than 16.5 g/dL in men and more than 16 g/dL in women, or a hematocrit level of more than 49% in men and more than 48% in women, or red cell mass > 25% above mean normal.
- Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent red cell, granulocytic white cell and platelet proliferation.
- Presence of JAK2V617F or JAK2 exon 12 mutation.
- While the minor criterion is:
- Serum erythropoietin level below the reference range for normal.
To diagnose polycythemia vera, all three major criteria must be fulfilled or the first 2 in addition to the minor criterion.
B) Imaging:


Radiological imaging has no role in the diagnosis of polycythemia. However, it can confirm the presence of an enlarged spleen.
The spleen is the main site of destruction of aged and deformed cells, and although the spleen isn’t always enlarged in polycythemia unlike myelofibrosis and chronic myeloid leukemia, it can cause severe discomfort to the patient.
Polycythemia vera treatment

Polycythemia is usually non-fatal in the short term. However, the main fatal complications that should be prioritized in treatment is the risk of blood clot formation and the transformation to myelofibrosis which may then transform to acute leukemia. Clinical presentation varies and therapy has to fit the patient’s needs and concentrate on the main symptoms that they have. Therefore, the main methods of therapy are:
- Reduction of the red cell mass to avoid the risk of clot formation (thrombosis) and ameliorate most of the symptoms.
- Decrease the rate of proliferation of red cells through the usage of chemotherapy.
- Optimally, the early and effective targeting of the genetic mutation is the most promising and successful way to control the disease.
- Control of hyperuricemia to avoid gouty arthritis and the risk of urinary uric acid stones or renal failure.
- Surgery if splenic enlargement is troublesome to the patient.
Most chemotherapy used in the management of the condition is highly toxic to the bone marrow and can even accelerate the transformation to acute leukemia. Therefore, they are not always used nowadays, except in cases when rapid reduction of hypercellularity is imperative. It is mostly completely avoided in old patients.
Medical therapy:
Medical therapy is the backbone of polycythemia treatment and it includes the following:
1) Phlebotomy

One of the oldest practices in medicine was bloodletting, which is inflicting a small wound on the patient and letting the blood flow. This primitive way was part of the ancient Hippocratic medicine and was found to be useless in most cases. Very few diseases, however, can benefit from this technique especially those associated with hyper-viscosity of the blood. A venous catheter is attached to the patient and blood is drained into a bag to help alleviate the symptoms of the patient and decrease the risk of thrombosis. Phlebotomy is performed one or two times a week.
A common question that must be hovering in your mind is whether or not blood collected from polycythemia patients allowed to be donated to blood banks, and there is no definite answer. Many blood banks still accept it, but this has greatly fell out of favor in many countries including the United States, not for a strictly medical reason but rather due to increased regulations to blood donating following the HIV pandemic in the 90s.
2) Aspirin

Aspirin in low doses helps prevent platelets from aggregating and is used in all patients with polycythemia except those with allergies to the substance or other medical contraindications. It can greatly reduce the risk of clot formation.
3) Cytoreductive chemotherapy

Phlebotomy is beneficial for reducing the risk of clot formation, but for those who are at high risk, Hydroxyurea is initiated. It acts on the DNA of cells killing them and reducing their number. It is effective for the rapid reduction of cellular count but comes with its share of side effects including increased risk of infections and on prolonged use, increased risk of leukemia.
4) JAK inhibitor drugs


As mentioned before, the main pathology is genetic, and solving the genetic mutation remains the optimal method of the therapy. Two drugs have been approved as JAK inhibitors for the treatment of polycythemia which are ruxolitinib and fedratinib. They are, however, only used in case of contraindications to hydroxyurea or failure of treatment. The reason behind that is that there is an increased risk of side effects such as anemia and severe platelet deficiency experienced in as much as fifth of patients receiving those drugs.Their main advantage is that they achieve greater and long-lasting effects compared to other drugs including reduction in the size of the spleen. It is also reported that fedaratinib can relieve myelofibrosis resulting from polycythemia.
5) H2 blockers

It is essential to protect patients against peptic ulcers. Many options exist for such purpose including proton pump inhibitors like omeprazole or H2 blockers like ranitidine.
6) Surgery


Two main complications occur due to polycythemia which need surgical treatment: splenic enlargement and Budd-Chiari syndrome. Splenic enlargement or splenomegaly can be troublesome if the spleen reaches a large size causing discomfort in the upper abdomen which is usually felt as heaviness. Also, due to the high probability of thrombus formation, splenic infarction can occur, causing sharp pain that may be repeated on several episodes.
Budd-Chiari syndrome is the obstruction of the hepatic veins draining the liver into the inferior vena cava and to the heart. It causes pain, abdominal enlargement due to ascites and liver enlargement. The condition is treated by the use of shunts to bypass the obstruction namely Trans jugular intrahepatic portosystemic shunt (TIPS), Side-to-side portocaval shunt or portocaval/cavoatrial shunt.
Outcome

Polycythemia vera is perhaps the most manageable of all myeloproliferative neoplasms with a 5-year survival rate of more than 80%. With appropriate treatment, a survival of about 14 years is expected, even for patients older than 60 years old. Younger patients are expected to live for more than 20 years.
The most troublesome fatal complications of polycythemia are its transformation to acute leukemia or blood clotting complications which can cause fatal heart attacks or pulmonary embolism.